
When a person passes so suddenly, it is almost always predicted they would ask for an autopsy report to be done. This is to know and to understand what could have caused it. In addition to that, it also answers the question who and why did it happen. It is also useful for the victim’s family and for people working in the medical field to understand the root of it. If you want to know more about autopsy reports and how they are written, I highly suggest you check out 8+ autopsy report examples in MS Word, Google Docs and PDF.
[bb_toc content=”][/bb_toc]
1. Autopsy Report Template
2. Autopsy Report Request Form
3. Request for Autopsy Report
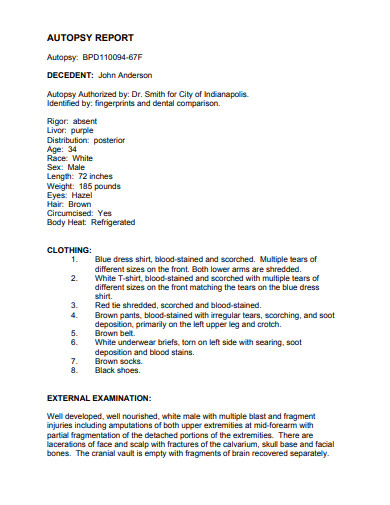
4. Printable Autopsy Report in PDF
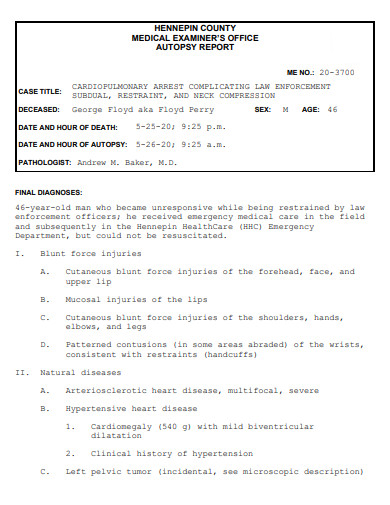
5. Medical Office Autopsy Report
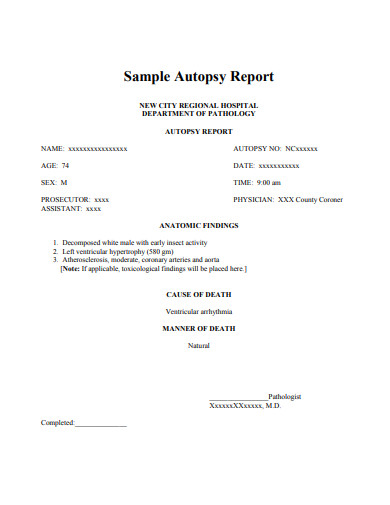
6. Sample Autopsy Report
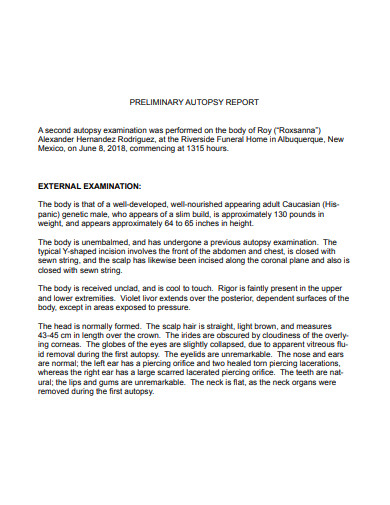
7. Preliminary Autopsy Report
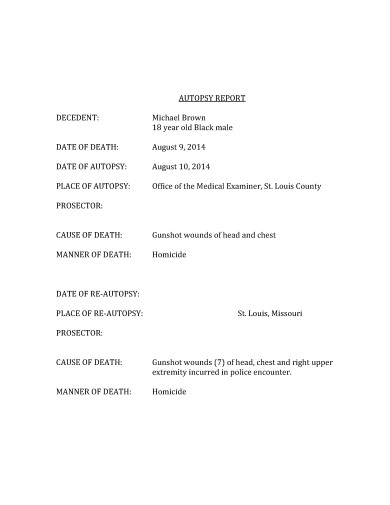
8. Formal Autopsy Report Template
9. Student Autopsy Report
What Is a Definition of Autopsy Report
An autopsy report is a written document that determines the cause of death of the victim. It contains several medical reports in lieu of the examination they took from the deceased. The document is only available to the immediate family of the said victim. It can also be available for the police to check if it helps with their investigation. A pathologist is the one responsible for performing an autopsy procedure.
Definition of Autopsy
An autopsy is an act of cutting open and examing a deceased body. This is so they can discover and understand the cause of death. It is a surgical procedure that consists of examining the corpse. In addition, an autopsy is performed to see and to know the root cause of the person’s untimely end. Lastly, it is also to determine if there were any other issues that could have caused a person’s life to end so shortly.
Definition of Report
A report is an act of describing something for information about a person. A spoken or written account about an event or a situation. A report is an act of investigating, observing an occurrence or incident in the form of a narrative. A report is an official account that is only presented as facts when the proof is given. Reports can range from mild to severe, depending on who reported.
Tools Used for Making Autopsy Reports
As we all know, there are types of autopsy reports. But there are also different types of tools or materials to use when you want to write an autopsy report. These reports may differ, but they all have one thing in common. They are used for filling out the information needed when you do your report. Check them out below.
- Forms
- Checklist
- Fill out
- Tick the box
- Essay
- Audio Recording
Types of Autopsy Reports
As you continue on to reading the article, here are some types of autopsy reports. Each type has its own use as well as its own definition. To know more about these, you may look below for the complete definition. Check it out right now.
- Complete autopsy – A complete autopsy is a process of examining the whole body of the deceased. Examining not only the external parts but the internal ones as well. A complete autopsy is more likely the most common type of autopsy report. This is what often happens if you wish to know the full length of the cause of death of the patient.
- Partial Autopsy – A partial autopsy is different from a complete autopsy. In a way that only the external part of the body is studied. This is the process of checking, examining and judging the cause of death by merely studying the external part. The internal part can be a part of the examination but is only limited to specific organs.
- Second Autopsy – Second autopsies happen when the deceased’s family asks for a second opinion. These types of autopsies are performed the second time around. However, asking for the original report from the first autopsy cannot be done. If you wish to know, you must examine the body again and see if there was any difference between the first and the current one. Only the family of the deceased is allowed to know.
- Observation Autopsy – From the name itself, it means to observe. This type of report is usually done with medical students. As this procedure is used for educational purposes. Wherein a pathologist performs the examination. The students simply watch how it is done.
- Exhumation Autopsy– Exhumation autopsy is the rarest type of autopsy. This is the type where a body has been dug up to be examined. To check or to recheck for things that may have been missed. Exhumation reports usually happen during crime investigations. However, this could also happen to almost anyone who wishes for this type of autopsy.
Tips for Writing an Autopsy Report
Are you planning on writing an autopsy report? Do you have any idea as to how it would look when it’s done? Are you told to write a good autopsy report after having been able to go through an observation autopsy? If you are hounded by these types of questions, no worries. Here are some tips to help you write a good autopsy report for any reason.
1. Write the Date
The date plays a crucial role when writing your report. This helps when you have to look for the day you examined a particular body. Dates also help you trace back to where you have made an error or have made a discovery. Writing dates should be the first few things to be seen.
2. Fill in the Necessary Details
Depending on which tool you might be using for your report, you need to fill out the necessary details. This includes the name of the deceased person, how they died, the cause of death and the date when they died. This is crucial to see if the deceased person’s body is still fresh enough to make a full autopsy report.
3. Add Your Name
By adding your name you are stating the fact you were the one to examine the body. This can also be used to trace who has examined the body. As well as your findings and the cause of death of the deceased. You are the only person who would know as you were the one examining it.
4. State the Nature of the Examination
State whether what examination you have done. By doing so, you are giving the correct information. A full autopsy, a partial autopsy, an observation, etc. This is also important information that needs to be written down for future reference.
5. Avoid Erasures
Avoiding erasures in your report. This is an official document. As much as possible, avoid having any erasures on your report. As people may assume you do not know what you are doing. If you are about to make a mistake, or a guess, write it down in a different paper before having to write it in your official report.
FAQs
What is the first thing to examine during an autopsy?
The autopsy usually begins by examining the external body.
How are we going to ensure that an autopsy report is accurate?
You may ask another pathologist to perform a second autopsy.
Are the reports confidential?
Yes. Only immediate family members are allowed to ask for the autopsy report. If you are not immediate family but you are also a family member, you may request for the autopsy report.
What do they do to the body after the autopsy report is completed?
When the autopsy report is finally completed, they will hand over the body back to the victim’s family. They are not allowed to keep it unless the victim’s family allows them to study the body for science.
Having to lose a person is always difficult. But to be able to understand and know the cause of their deaths can bring a glimmer of hope. Autopsy reports do just that. They tell you the cause was either natural or man-made. When you write your autopsy report, always remember that even the smallest of details are important.